We hear a lot about stress, but what is it? Taber’s Cyclopedia Medical Dictionary defines stress as “the result produced when a structure, system or organism is acted upon by forces that disrupt equilibrium or produce strain”. In simpler terms, stress is the result of any emotional, physical, social, economic, or other factors that require a response or change. It is generally believed that some stress is okay (sometimes referred to as “challenge” or “positive stress”) but when stress occurs in amounts that you cannot handle, both mental and physical changes may occur.
“Workplace stress” then is the harmful physical and emotional responses that can happen when there is a conflict between job demands on the employee and the amount of control an employee has over meeting these demands. In general, the combination of high demands in a job and a low amount of control over the situation can lead to stress.
Stress in the workplace can have many origins or come from one single event. It can impact on both employees and employers alike.
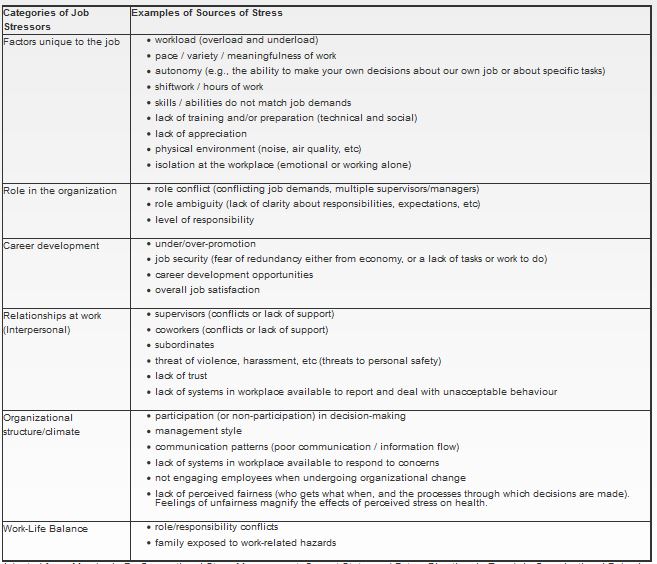
Cause stress at the workplace:
In the workplace, stress can be the result of any number of situations. Some examples include:
Stress cause health effects:
Yes, stress can have an impact on your overall health. Our bodies are designed, pre-programmed if you wish, with a set of automatic responses to deal with stress. This system is very effective for the short term “fight or flight” responses we need when faced with an immediate danger. The problem is that our bodies deal with all types of stress in the same way. Experiencing stress for long periods of time (such as lower level but constant stressors at work) will activate this system, but it doesn’t get the chance to “turn off”. The body’s “pre-programmed” response to stress has been called the “Generalized Stress Response” and includes:
- increased blood pressure.
- increased metabolism (e.g., faster heartbeat, faster respiration).
- decrease in protein synthesis, intestinal movement (digestion), immune and allergic response systems.
- increased cholesterol and fatty acids in blood for energy production systems.
- localized inflammation (redness, swelling, heat and pain).
- faster blood clotting.
- increased production of blood sugar for energy.
- increased stomach acids.
From: Basic Certification Training Program: Participant’s Manual, Copyright© 2006 by the Workplace Safety and Insurance Board of Ontario.
Stress can contribute to accidents/injuries by causing people to:
- sleep badly.
- over-medicate themselves and/or drink excessively.
- feel depressed.
- feel anxious, jittery and nervous.
- feel angry and reckless (often due to a sense of unfairness or injustice).
When people engage in these behaviours or are in these emotional states, they are more likely to:
- become momentarily (but dangerously) distracted
- make errors in judgment.
- put their bodies under physical stress, increasing the potential for strains and sprains.
- fail in normal activities that require hand-eye or foot-eye coordination.
Stress can also lead to accidents or injuries directly by not giving the person the control necessary to stop the threat to their physical well-being.
Luckily, there are usually a number of warning signs that help indicate when you are having trouble coping with stress before any severe signs become apparent. These signs are listed below.
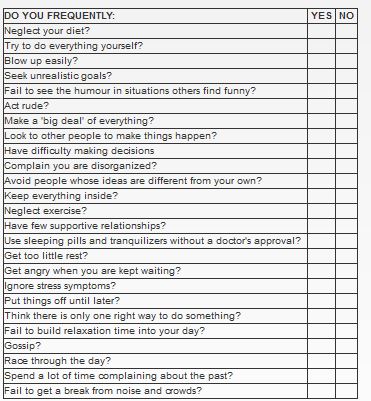
Interpretation of your score (based on the number of “Yes” selections):
0-5: There are few hassles in your life. Make sure though, that you are not trying to deliberately avoid problems.
6-10: You’ve got your life in fairly good control. Work on the choices and habits that could still be causing you some unnecessary stress in your life.
11-15: You are approaching the danger zone. You may be suffering stress-related symptoms and your relationships could be strained. Think carefully about choices you’ve made and take relaxation breaks every day.
16-25: Emergency! It is critical that you stop and re-think how you are living; change your attitudes and pay careful attention to diet, exercise and relaxation.
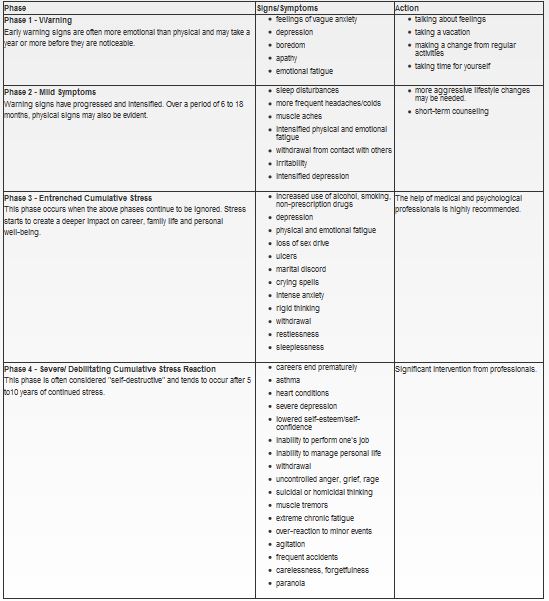
Signs or symptoms happen all at once and what level of help should be sought?
No, not normally. The signs and symptoms from stress tend to progress through several phases or stages. The phases can be described as below:
Improve my overall mental health:
Good mental health helps us to achieve balance and cope with stressful times.
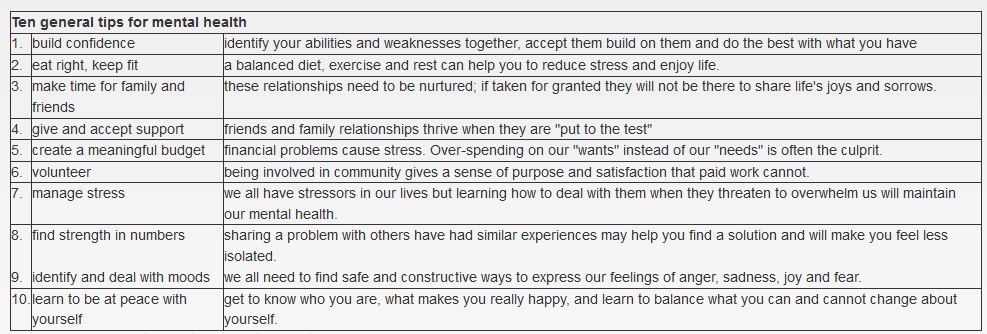
Other mental fitness tips include:
- Give yourself permission to take a break from your worries and concerns. Recognize that dedicating even a short time every day to your mental fitness will reap significant benefits in terms of feeling rejuvenated and more confident.
- “Collect” positive emotional moments – Make a point of recalling times when you have experienced pleasure, comfort, tenderness, confidence or other positive things.
- Do one thing at a time – Be “present” in the moment, whether out for a walk or spending time with friends, turn off your cell phone and your mental “to do” list.
- Enjoy hobbies – Hobbies can bring balance to your life by allowing you to do something you enjoy because you want to do it.
- Set personal goals – Goals don’t have to be ambitious. They could be as simple as finishing a book, walking around the block every day, learning to play bridge, or calling your friends instead of waiting by the phone. Whatever goal you set, reaching it will build confidence and a sense of satisfaction.
- Express yourself – Whether in a journal or talking to a wall, expressing yourself after a stressful day can help you gain perspective, release tension, and boost your body’s resistance to illness.
- Laugh – Laughter often really is the best medicine. Even better is sharing something that makes you smile or laugh with someone you know.
- Treat yourself well – Take some “you” time – whether it’s cooking a good meal, having a bubble bath or seeing a movie, do something that brings you joy.